
Retinal Detachment (RD) repair is one of the most common procedures preformed by retina surgeons. Eyes known to have a substantial risk for retinal detachment include the fellow eye or second eye of someone who has experienced retinal detachment in one eye. Any one who has had cataract surgery has a modestly increased risk of retinal detachment and their risk increases slightly if they have also had a secondary laser procedure known as YAG capsulotomy. Extremely nearsighted (myopic) eyes, eyes with lattice degeneration and people with Marfan’s syndrome are also conditions associated with a higher risk.
A retinal detachment occurs when a defect is formed in the retina. The defect is an opening in the retina that allows fluid to lift the thin retinal tissue away from its normal blood supply. Best results for return of vision occur when the condition is detected early and remedied.
Prophylaxis Retinal Detachment Laser Photocoagulation may successfully prevent further RD when the tear or hole is detected early before a large area of retina has become detached. A Focal Laser procedure seals the hole or tears thereby preventing normal intraocular fluid from entering the subretinal space detaching the retina.
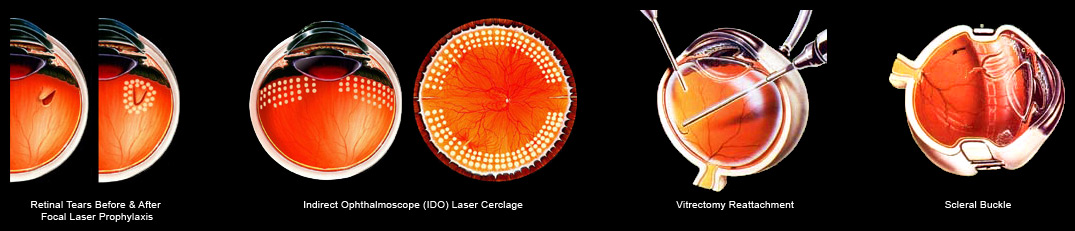
360° Laser Cerclage is a preventative procedure applied in the peripheral area of retina where an estimated 95% retinal breaks which cause retinal detachment occur. This procedure was developed by Helen Keller Foundation for Research and Education’s researchers associated with Retina Specialists of Alabama. This procedure is done even in the absence of a retinal defect in the high risk categories listed above. A bond is formed in the peripheral circumference of the entire retina. Should a break occur in the most common area the treated bond prevents the retina from detaching into the all important areas of the retina where detail vision occurs.
Vitrectomy, an intraocular microscopic surgery, is the major surgical option for repairing retinal detachments. A number of advanced techniques may be employed once the vitreous gel is removed by vitrectomy from the interior globe of the eye allowing direct access to the retina. Laser procedures as those described above and/or the insertion of temporary implants of air, gas, or silicone oil are employed to repair and support the retina against its blood supply while the retina heals. In the past an external support, a scleral buckle, was used but more often now the internal implants are the first choice. The air and gases dissipate on their own in time but silicone oil requires an additional procedure to remove the oil once the retina is secure and no further threat of redetachment exists.
Your surgeon will give you lots of information about your specific procedures and what you may expect. There are a large number of personnel dedicated to your successful experience and restoration of your vision. Both the surgeon’s office staff and the hospital staff are in your corner. The surgeon will depend on you to follow specific instructions regarding the care of your eye, to monitor your vision and to report your symptoms.